
The age-adjusted incidence rate for meningioma, the most common non-malignant brain tumor, increased from about 6.3 per 100,000 in 2004 to about 7.8 per 100,000 in 2009 before leveling off (through 2011).
The annual percentage increase between 2004 and 2009 was 2.4% per year. The annual increase was significant for males and females, whites and blacks, and non-Hispanics. Although the incidence of these tumors increased for all age groups except 0-19, the increase was statistically significant only for 45-54 years of age and 65 and older.
The case-control research that has examined the association between long-term use of mobile phones and risk of meningioma has yielded mixed results. Some studies have found a significant association whereas others have not.
---
---
Dolecek TA, Dressler EV, Thakkar JP, Liu M, Al-Qaisi A, Villano JL. Epidemiology of meningiomas post-Public Law 107-206: The Benign Brain Tumor Cancer Registries Amendment Act. Cancer. 2015 Apr 14. doi: 10.1002/cncr.29379. [Epub ahead of print]
Abstract
BACKGROUND: The current analysis follows the implementation of Public Law 107-260, the Benign Brain Tumor Cancer Registries Amendment Act, which mandated the collection of nonmalignant brain tumors.
METHODS: Meningiomas were selected from the Surveillance, Epidemiology, and End Results (SEER) Program database for the years 2004 to 2011. Demographic and clinical characteristics, initial treatment patterns, and survival outcomes were evaluated using surveillance epidemiology statistical methods.
RESULTS: The average annual age-adjusted incidence rate per 100,000 population was 7.62 (95 % confidence interval [CI], 7.55-7.68) for all meningiomas, 7.18 (95% CI, 7.12-7.25) for benign meningiomas, 0.32 (95% CI, 0.31-0.33) for borderline malignant meningiomas, and 0.12 (95% CI, 0.11-0.12) for malignant meningiomas. The annual rates increased for benign and borderline malignant tumors but decreased for malignant tumors. The rates for women exceeded those for men, especially for those with benign meningiomas. Black race was associated with significantly higher rates as was advancing age. Greater than 80% of tumors were located in cerebral meninges. Diagnostic confirmation through pathology occurred for approximately 50% of benign tumors, 90% of borderline malignant tumors, and 80% of malignant tumors. No initial treatment was reported for greater than 60% of benign tumors, 29% of borderline malignant tumors, or 31% of malignant tumors. The 5-year relative survival estimates for benign tumors, borderline malignant tumors, and malignant tumors were 85.6% (95% confidence interval [CI], 85%-86.2%), 82.3% (95% CI, 79.3%-84.8%), and 66% (95% CI, 60.6%-70.9%), respectively. Predictors of poorer survival were advanced age, being male gender, black race, no initial treatment, and malignant tumor behavior.
CONCLUSIONS: The current analysis demonstrates that there is an increasing incidence.
Abstract
BACKGROUND: The current analysis follows the implementation of Public Law 107-260, the Benign Brain Tumor Cancer Registries Amendment Act, which mandated the collection of nonmalignant brain tumors.
METHODS: Meningiomas were selected from the Surveillance, Epidemiology, and End Results (SEER) Program database for the years 2004 to 2011. Demographic and clinical characteristics, initial treatment patterns, and survival outcomes were evaluated using surveillance epidemiology statistical methods.
RESULTS: The average annual age-adjusted incidence rate per 100,000 population was 7.62 (95 % confidence interval [CI], 7.55-7.68) for all meningiomas, 7.18 (95% CI, 7.12-7.25) for benign meningiomas, 0.32 (95% CI, 0.31-0.33) for borderline malignant meningiomas, and 0.12 (95% CI, 0.11-0.12) for malignant meningiomas. The annual rates increased for benign and borderline malignant tumors but decreased for malignant tumors. The rates for women exceeded those for men, especially for those with benign meningiomas. Black race was associated with significantly higher rates as was advancing age. Greater than 80% of tumors were located in cerebral meninges. Diagnostic confirmation through pathology occurred for approximately 50% of benign tumors, 90% of borderline malignant tumors, and 80% of malignant tumors. No initial treatment was reported for greater than 60% of benign tumors, 29% of borderline malignant tumors, or 31% of malignant tumors. The 5-year relative survival estimates for benign tumors, borderline malignant tumors, and malignant tumors were 85.6% (95% confidence interval [CI], 85%-86.2%), 82.3% (95% CI, 79.3%-84.8%), and 66% (95% CI, 60.6%-70.9%), respectively. Predictors of poorer survival were advanced age, being male gender, black race, no initial treatment, and malignant tumor behavior.
CONCLUSIONS: The current analysis demonstrates that there is an increasing incidence.
Excerpts
Population-based studies of meningiomas have been limited because of the benign nature of the histology; and, before diagnosis year 2004, state central cancer registries were not required to collect nonmalignant cases. That changed with the passage of Public Law 107-260, the Benign Brain Tumor Cancer Registries Amendment Act.1 This law mandated the collection of benign and borderline malignant brain tumors beginning with diagnosis year 2004. Our analysis on this common but understudied tumor follows the implementation of this law ...
Meningiomas have the highest incidence rate among all primary brain and central nervous system (CNS) tumors. Nonmalignant meningioma is the most frequently reported histology, accounting for >33% of all primary brain and CNS tumors.
We evaluated population-based data from the Surveillance, Epidemiology, and End Results (SEER) Program 18 registries of the National Cancer Institute. The SEER Program is an authoritative source of cancer incidence and survival in the United States with registries that cover approximately 28% of the US population. Although Public Law 107-260 only applies to state-wide registries, SEER has voluntarily agreed to collect nonmalignant brain tumor data in accordance with the mandate.
In total, 51,065 new meningiomas occurred in the 18 SEER geographic areas during the period from 2004 to 2011. Of these tumors, 50,290 (>98%) were determined to be nonmalignant (benign or borderline malignant) and were collected under the mandate of Public Law 107-260. Greater than 95% of these tumors were benign, and the remaining tumors were classified as borderline malignancies. Only 775 malignant tumors were diagnosed during the 8 study years.
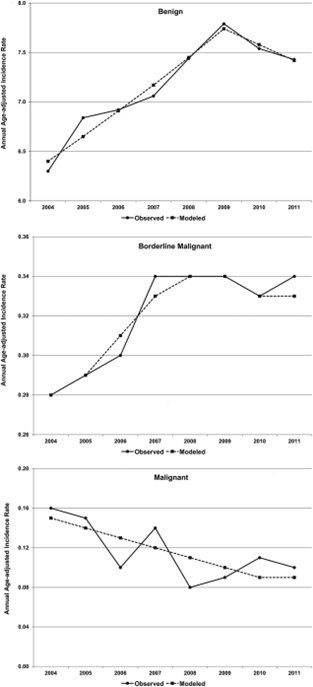
... Statistically significant increases in the annual AAIRs from 2004 to 2011 were apparent for benign and borderline malignant tumors, whereas AAIRs for malignant tumors significantly decreased....
... Statistically significant increases were observed from 2004 to 2009 for benign meningiomas (APC, 3.86; P<.05), with a leveling off and no significant change in AAIRs during 2009 to 2011. The pattern for borderline malignant meningiomas was similar, but the significant increase appeared from 2004 to 2008 (APC, 5.50; P<.05), with no significant change over the years from 2008 to 2011. No joinpoint was apparent for malignant meningiomas, but a significant linear decline (APC, 27.27; P<.05) was observed.
Rising risk over the study period very well may have been an artifact of increasingly accurate reporting associated with implementation of the law. The extent to which this contributed to the increased incidence is unknown. There is also a degree of ascertainment bias because of improving diagnostic techniques, because 50% of patients with benign tumors were registered based on imaging versus pathology, which is required for most other cancers ...
Population-based studies of meningiomas have been limited because of the benign nature of the histology; and, before diagnosis year 2004, state central cancer registries were not required to collect nonmalignant cases. That changed with the passage of Public Law 107-260, the Benign Brain Tumor Cancer Registries Amendment Act.1 This law mandated the collection of benign and borderline malignant brain tumors beginning with diagnosis year 2004. Our analysis on this common but understudied tumor follows the implementation of this law ...
Meningiomas have the highest incidence rate among all primary brain and central nervous system (CNS) tumors. Nonmalignant meningioma is the most frequently reported histology, accounting for >33% of all primary brain and CNS tumors.
We evaluated population-based data from the Surveillance, Epidemiology, and End Results (SEER) Program 18 registries of the National Cancer Institute. The SEER Program is an authoritative source of cancer incidence and survival in the United States with registries that cover approximately 28% of the US population. Although Public Law 107-260 only applies to state-wide registries, SEER has voluntarily agreed to collect nonmalignant brain tumor data in accordance with the mandate.
In total, 51,065 new meningiomas occurred in the 18 SEER geographic areas during the period from 2004 to 2011. Of these tumors, 50,290 (>98%) were determined to be nonmalignant (benign or borderline malignant) and were collected under the mandate of Public Law 107-260. Greater than 95% of these tumors were benign, and the remaining tumors were classified as borderline malignancies. Only 775 malignant tumors were diagnosed during the 8 study years.
... Statistically significant increases in the annual AAIRs from 2004 to 2011 were apparent for benign and borderline malignant tumors, whereas AAIRs for malignant tumors significantly decreased....
... Statistically significant increases were observed from 2004 to 2009 for benign meningiomas (APC, 3.86; P<.05), with a leveling off and no significant change in AAIRs during 2009 to 2011. The pattern for borderline malignant meningiomas was similar, but the significant increase appeared from 2004 to 2008 (APC, 5.50; P<.05), with no significant change over the years from 2008 to 2011. No joinpoint was apparent for malignant meningiomas, but a significant linear decline (APC, 27.27; P<.05) was observed.
The piece-wise regression trend analyses suggest that benign meningioma rates stabilized at diagnosis year 2009 and had no significant change from 2009 to 2011. Reporting for the diagnosis years 2004 through 2009 may have been influenced by the many factors discussed above, and diagnosis years 2009 through 2011 actually may reflect accurate incidence estimates for meningiomas with more complete registration of nonmalignant tumors ...
Conclusions
The implementation of the Benign Brain Tumor Cancer Registries Amendment Act, Public Law 107-260, afforded an opportunity to gain a better understanding and new insights into nonmalignant brain tumors. This legislative contribution has distinctive relevance to patients with meningioma, because it is known as the most common CNS tumor in which the vast major of patients present with benign histologies. Our current analysis after the implementation of Public Law 107-260 in diagnosis year 2004 demonstrates increasing incidence rates of nonmalignant meningiomas that stabilized around 2009. This trend was undoubtedly because of learning curves associated with registration procedures put into practice to comply with the law. The period of rate stabilization likely reflects meningioma estimates that are closer to its true incidence with more precise behavior classifications in the SEER registries data. Our report, for which we used this improved, high-quality cancer registry data set on brain tumors, represents the most current population-based description of the demographic and clinical characteristics, initial treatment patterns, and survival outcomes for patients with nonmalignant and malignant meningiomas.
Conclusions
The implementation of the Benign Brain Tumor Cancer Registries Amendment Act, Public Law 107-260, afforded an opportunity to gain a better understanding and new insights into nonmalignant brain tumors. This legislative contribution has distinctive relevance to patients with meningioma, because it is known as the most common CNS tumor in which the vast major of patients present with benign histologies. Our current analysis after the implementation of Public Law 107-260 in diagnosis year 2004 demonstrates increasing incidence rates of nonmalignant meningiomas that stabilized around 2009. This trend was undoubtedly because of learning curves associated with registration procedures put into practice to comply with the law. The period of rate stabilization likely reflects meningioma estimates that are closer to its true incidence with more precise behavior classifications in the SEER registries data. Our report, for which we used this improved, high-quality cancer registry data set on brain tumors, represents the most current population-based description of the demographic and clinical characteristics, initial treatment patterns, and survival outcomes for patients with nonmalignant and malignant meningiomas.
source: http://bit.ly/2mZBsdH
